Fluoxetine
"Generic fluoxetine 10 mg online, women's health clinic edmonton hours."
By: Karen Patton Alexander, MD
- Professor of Medicine
- Member in the Duke Clinical Research Institute

https://medicine.duke.edu/faculty/karen-patton-alexander-md
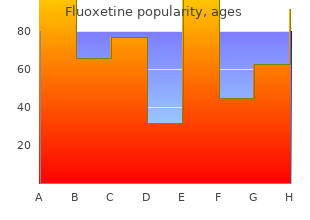
In each panel discount generic fluoxetine uk menstrual like cramps at 37 weeks, any two vertical bars not identified by the same letter represent statistically different values (p<0 buy fluoxetine online from canada breast cancer gift ideas. What the precise molecular mechanisms are cannot be determined from these results discount fluoxetine 20mg without prescription menstruation hormonal changes. Further research into the aromatization products (estrogens) and opioid peptide pathways involved may produce new insights, as there is good evi- dence that the former (Ho et al. The interrelationships of steroids, growth hormone, and other hormones on pubertal growth. Alteration of pulsatile growth hormone secretion by growth-inducing exercise: Involvement of endogenous opiates and somatostatin. The effect of androgens on the pulsatile release and the twenty-four hour mean concentration of growth hormone in peripubertal males. Chronic sex steroid exposure increases mean plasma growth hormone concentration and pulse amplitude in men with isolated hypogonadotropic hypogonadism. Alterations in the pulsatile properties of circulating growth hormone concentrations during puberty in boys. Augmentation of growth hormone secretion during puberty; evidence for a pulse amplitude-modulated phenomenon. Physiologic testosterone or estradiol induction of puberty increases plasma somatomedin C. Clinical longitudinal standards for height and height velocity for North American children. Cluster analysis: A simple, versatile, and robust algorithm for endocrine pulse detection. Role of endogenous opiates in the expression of negative feedback actions of androgen and estrogen on pulsatile properties of luteinizing hormone secretion in man. Miss Ginger Bauler, Catherine Kern, and Beth Epstein of the Core Radiological Assay Laboratory performed most of the immunoassays. Most of the short-term physiologic effects in adult males are transitory (Haupt and Rovere 1984; Wright 1980; Yesalis et al. Other psychological effects of use, that is, increased confidence, euphoria, and enhanced libido (Wright 1980; Haupt and Rovere 1984; Rahrke et al. However, these effects, like the physical outcomes, diminish when use is discontinued (Wright 1978; Wright 1982) and may in fact turn into frank depression (Pope and Katz 1988). Such reductions may be associated, therefore, more with a psychological than a physical motivation for continued cyclical use of the drugs. It is possible that the psychological or affective outcomes act as secondary reinforcers, equally as powerful as the primary physical ones. In this chapter, data from that survey are discussed in relation to psychological rewards of use and the potential for dependence to develop. In particular, the relationships between age of initiation of use, frequency of use, methods of administration, unwillingness to discontinue use, and perceptions of strength, health, and peer use are examined. It also appears that the development of drug-use patterns, including acquisition and habit forma- tion, for various substances is most likely to occur between 11 and 24 years of age (Pandina et al. The outcomes of use behaviors, from initia- tion of use through possible dependence on drugs, are of concern for both their physical and psychological consequences. Adolescence is an age period during which a number of major developmental tasks are addressed (Adelson 1980). Recreational drugs, both licit and illicit, generally are expected to provide pleasurable effects for the user, with mood-altering capabilities most valued (Johnston et al. Not uncommonly, problems in personal, family, school, and peer domains are identified as causative or contributing to drug use, along with the interactions between these and other contexts,. Drug treatment programs recognize that physical dependence on most drugs can be relatively easily reduced, but eliminating psychological dependence is more difficult, although necessary for total recovery. One such attitude is a tendency to over- look, disbelieve, or argue against the physical risks of drug use and to per- ceive the benefits as outweighing the risks. Drug use continues, at various levels, as long as the perceived benefits, often real as well, outweigh the perceived and equally real problems associ- ated with use. Research also indicates that a general tendency to take risks is associated with the development of drug abuse (Crowley 1988). Adolescent substance users usually overestimate the prevalence and accepta- bility of use by their peers (Sherman et al. A strong predictor of an individual’s use of drugs is reported use by a friend or admired other (Hansen et al.
The analytic framework (Figure A) shows the target population generic 20mg fluoxetine with visa pregnancy rhinitis, interventions and outcomes that were examined generic fluoxetine 10mg visa women's health center uga. Comparisons of interest include: a) Catheter ablation compared with medical therapy b) Comparing ablation using different energy sources Key Question 2 buy generic fluoxetine on-line menstrual 45 days. Comparisons of interest include: a) Catheter ablation compared with medical therapy b) Comparing ablation using different energy sources Key Question 3. Analytic framework for catheter ablation for atrial fibrillation *Patients with longstanding persistent atrial fibrillation, persistent atrial fibrillation, or paroxysmal atrial fibrillation (considered separately); includes general population and Medicare population. The Key Informant panel included experts in cardiology primarily (with specialties in electrophysiology, heart failure, and cardiovascular aging/cardiovascular disease in older adults) and internal medicine; representatives from relevant specialty societies; government representatives. The final topic refinement document served as the basis for the review protocol with minor changes. Key Informant input during topic refinement confirmed that this was a logical approach. Reference lists of included articles and relevant review articles were inspected for relevant ® publications. All citations were reviewed independently by two individuals at both the title/abstract and full-text level and differences were resolved by consensus. For all Key Questions, the focus was on evidence from comparative studies with the least potential for bias. Comparative observational studies were required to have a minimum of 100 patients to be included. Registry and administrative data studies were considered if inclusion criteria were met. Comparisons of different techniques and/or approaches and mapping were beyond the scope of this report and thus were excluded. For Key Question 2, case series that were specifically designed to evaluate harms and/or adverse events following ablation, had a minimum of 1000 patients and at least 80 percent followup were included because all included comparative studies were relatively small in size. Including these large case series of ablation patients allowed for the calculation of risk estimates of adverse events based on a larger number of patients. For all Key Questions, both long-term (>12 months) and short-term (≤12 months) outcomes were reported. The primary outcomes (see Rating the Body of Evidence below) were considered to be the most clinically important and were the focus of reporting, decisions for data pooling and determination of overall strength of evidence. Additional outcomes are reported in the detailed evidence synthesis sections of the Key Questions with a focus on outcomes common across studies. Where applicable and where data were available, results from short-term (≤12 months) and long-term (>12 months) followup were described. Studies published only as conference abstracts, non-English-language articles, and studies of nonhuman subjects were excluded. All citations found to be potentially appropriate for inclusion by either reviewer underwent full-text review. Each full-text article was independently evaluated for final inclusion by two investigators. After data extraction, at least one other staff member and one study investigator each verified the accuracy and completeness of abstraction for each study included. Comparative observational studies were assessed for study design features and sources of potential bias. Two investigators independently assessed the quality of each study, and any discrepancies were resolved through discussion and consensus. Studies rated “good” are considered to have the least risk of bias and their results are considered valid. Good-quality studies include clear descriptions of the population, setting, interventions, and comparison groups; a valid method for allocation of patients to treatment; low dropout rates and clear reporting of dropouts; appropriate means for preventing bias; and appropriate measurement of outcomes. Studies rated “fair” are susceptible to some bias, though not enough to invalidate the results. These studies may not meet all the criteria for a rating of good quality, but no flaw is likely to cause major bias. The study may be missing information, making it difficult to assess limitations and potential problems. The fair-quality category is broad, and studies with this rating will vary in their strengths and weaknesses. The results of some fair-quality studies are likely to be valid, while others may be only possibly valid.
Verapamil and diltiazem should be used with caution in patients receiving intravenous beta-blockers discount 10mg fluoxetine mastercard women's health green coffee, those with congestive heart failure and those taking oral quinidine 20mg fluoxetine otc breast cancer inspirational quotes. It is preferred by most cardiologists for sustained ventricular tachycardia causing hemodynamic compromise buy fluoxetine 20 mg with visa pregnancy jokes cartoons. Some ventricular tachycardias can be caused or exacerbated by bradycardia or heart block. In the presence of high-grade heart block, antiarrhythmic drugs can cause cardiac standstill. When high-grade heart block is present, therefore, a temporary pacemaker should be inserted before using antiarrhythmic drugs; pacing may abolish the arrhythmia. When a drug must be used in the presence of heart block, lidocaine is least likely to increase the block. Defibrillation is the treatment of choice; drugs are for prevention of recurrence. In the presence of heart block not associated with atrial tachycardia, potassium should be withheld if the serum concentration is greater than 4. The drug can cause bradyarrhythmias Adverse Effects – Severe adverse effects, particularly requiring implantation of a permanent pacemaker (V pulmonary toxicity, can occur with usual doses of Essebag et al, J Am Coll Cardiol 2003; 41:249). Because of its adverse effects, other increased hepatic enzyme activity are common; cir- drugs are often used first, particularly in younger rhosis and fatal hepatic necrosis have been reported. Blue- toxicity of digoxin, diltiazem, quinidine, pro- Treatment Guidelines from the Medical Letter • Vol. Although it can cause heart block, hypoten- farin and other drugs (see the Medical Letter Adverse sion, transient atrial fibrillation, non-sustained ventric- Drug Interactions Program). Esmolol is an intravenous cardioselective dioverter-defibrillators, use of sotalol reduced the risk agent with an elimination half-life of about nine min- of death from any cause or delivery of a first shock for utes; it is effective in controlling the ventricular any reason (A Pacifico et al, N Engl J Med 1999; response in atrial flutter or fibrillation, particularly after 340:1855). The in terminating and preventing recurrences of many major risk is torsades de pointes, which occurred in supraventricular tachycardias and slowing the ventric- 0. Either other drugs (see the Medical Letter Adverse Drug diltiazem or verapamil can raise serum digoxin levels, Interactions Program). Whether drug-induced torsades de pointes and in some arrhyth- propafenone, which also has beta-blocking activity in mias related to digitalis toxicity. It is effective in about 60% of patients with nodal blocking agent such as digoxin, verapamil or a atrial flutter and 30% with atrial fibrillation. Propafenone can increase serum digoxin Lidocaine (Xylocaine, and others), which is only concentrations to toxic levels. Clearance of the drug drugs are only used occasionally now, mainly in often decreases during therapy; monitoring plasma patients not tolerating other agents. The prac- concentrations to potentially toxic levels, and it also tice of giving lidocaine prophylactically to patients interacts with many other drugs (see the Medical with suspected acute myocardial infarction has been Letter Adverse Drug Interactions Program). With long-term use, adverse extracardiac effects, mias causing cardiac arrest (Guidelines, Circulation such as fever or rash, are fairly common. Nausea and months of therapy, and up to 30% develop a lupus-like tremor are common, but may be reduced when the syndrome, which usually disappears slowly when the drug is given with food. Should not be used in patients with congestive heart failure or ischemic heart disease. Subscription Services Mailing Address Subscriptions Permissions the Medical Letter is an independent the Medical Letter, Inc. Copyright and Disclaimer Call: 800-211-2769 or 914-235-0500 No part of the material may be reproduced or relies on a review of published and M-F 8am-6pm Eastern Time Bulk Subscriptions transmitted by any process in whole or in part unpublished literature, with an emphasis Fax: 914-632-1733 Special reduced rates for bulk without prior permission in writing. The editors on controlled clinical trials, and on the Email: custserv@medicalletter. Contact Customer and publisher do not warrant that all the mate- opinions of its consultants. Special rial in this publication is accurate and complete Letter is supported solely by subscription Web Site Classroom rates are available. The Editors and Publisher Site license inquires to: declare no conflict of interest. Your heartbeat starts in the top of your heart in the sinus Your heart’s upper chambers (atria) take in the blood from node.
Cheap fluoxetine 10mg on line. What Women Want | Isis Mckay.
References:
- https://www.jqcjc.org/documents/v6i1.pdf
- https://www.openaccessjournals.com/articles/an-evidencebased-approach-to-conducting-clinical-trial-feasibility-assessments.pdf
- http://dro.dur.ac.uk/20987/1/20987.pdf?DDD29+hsmz78+d700tmt
- https://nett.umich.edu/sites/default/files/docs/ctmc_webinar_trial_management_09.15.2017.pdf